
OPEN ENROLLMENT IS NOW!
Complete your enrollment for 2025 today and ensure you are fully covered before open enrollment ends!
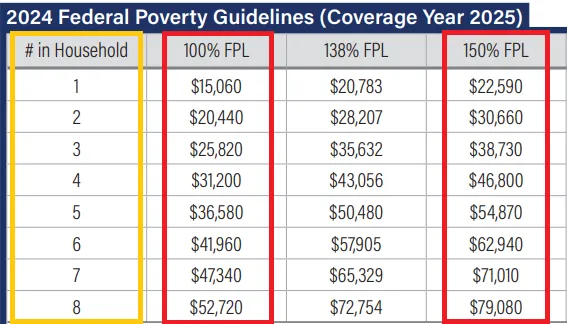
If your income for you/your family size falls within the ranges below, you can qualify for a $0 Health-Plan for 2025!
Current Contracted Carriers
(Not all carriers are shown below)

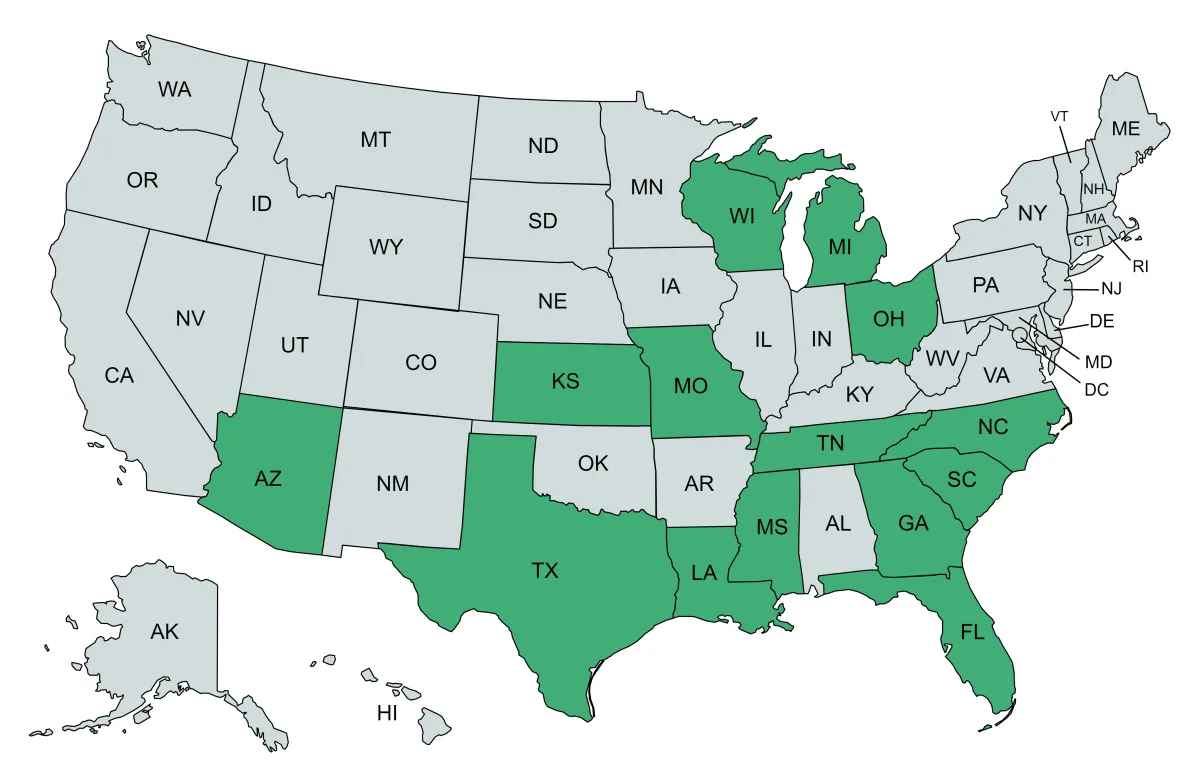
Current States We Service
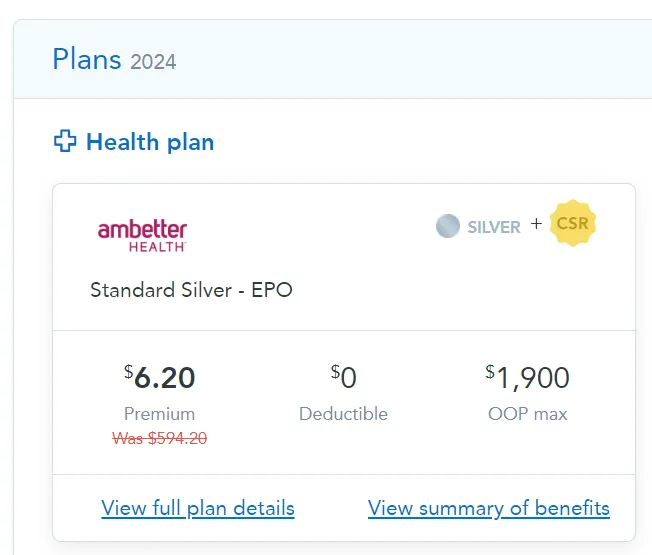
Previous Client's Insurance Examples!
(Plans shown below may not be available in your exact state/zip code)
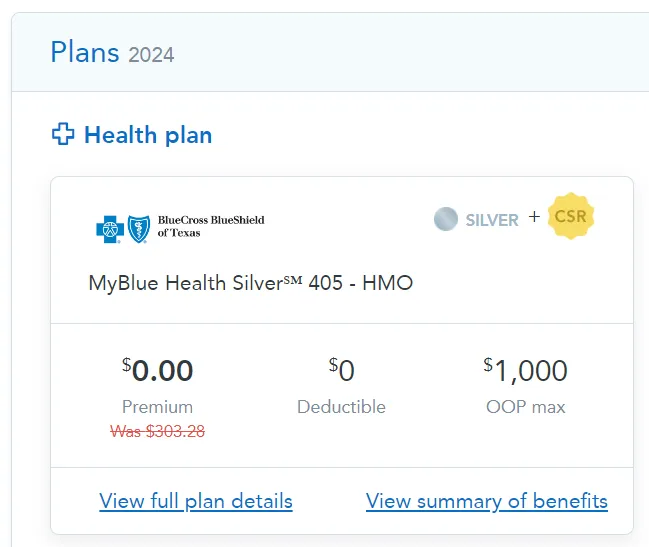
Texas, 78521 Zip Code
2 Person Household
$21,900/Yr Annual Household Income
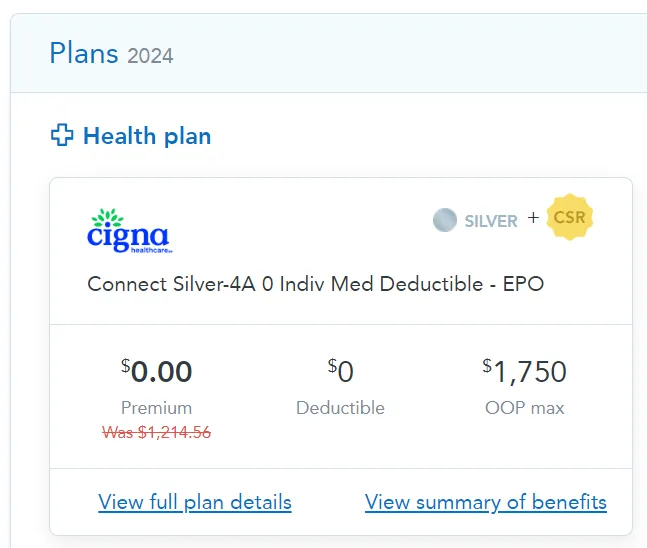
Tennessee, 38357 Zip Code
1 Person Household
$19,800/Yr Annual Household Income
Louisiana, 70062 Zip Code
1 Person Household
$21,200/Yr Annual Household Income

Louisiana, 70517 Zip Code
2 Person Household
$43,000/Yr Annual Household Income
Copyright 2026 . All rights reserved
Privacy Policy
Data Collection: Our Agents collect Personally Identifiable Information (PII) solely for the purposes mentioned in our Comprehensive Attestation Agreement.
Data Protection: We are committed to ensuring the privacy and safety of your PII. Your data will not be shared for any purposes other than those explicitly stated in our agreement.
Income Attestation: We use your income information solely to determine eligibility for health insurance programs and potential subsidies.
Terms of Service
By using our services, you agree to the following terms:
Representation: You grant the authorized agent, as mentioned in the attestation disclaimer, the authority to act on your behalf concerning health insurance matters, including enrollment, renewals, and related decisions.
Accuracy: You confirm that all information provided is true and accurate. False or misleading information can lead to the termination of services.
Revocation: Your consent remains in effect until you revoke it. You may revoke or modify your consent at any time.
Limitation of Liability: The authorized agent and associated entities are not liable for any errors or omissions in the services provided or for any damages, including indirect or consequential damages.
TCPA Disclaimer
By providing your phone number, you expressly consent to receive auto-dialed and/or pre-recorded telemarketing calls, text messages, and/or emails from the authorized agent mentioned in the attestation disclaimer at the phone number and email address you provided, including for marketing purposes.
You understand that consent is not a condition of purchase.
Message and data rates may apply.